Most are aware of the obesity epidemic and associate obesity to be the result of an increase in body fat. The World Health Organisation monitors population trends in obesity by body mass index or BMI (BMI= bodymass (kg)/ height (m)2). Normal, or ‘healthy’, BMI ranges from 18.5 to 25 kg/m2 with overweight and obese being > 25 and 30 kg/m2, respectively. Whilst many researchers question the validity of BMI as a an index of body fat, longitudinal trends in BMI show a continual rise in the overweight and obese to a point that 2/3rds of the population is deemed to either overweight or obese – a change in the human phenotype that questions what is ‘normal’ in Ireland today!
A rise in total body fat, and regional fat deposited around the abdomen, is highly associated risk to the major causes of mortality and morbidity, in particular heart disease and type II diabetes. Because BMI is only a ‘rough guide’ to the amount of body fat, it follows that interventions designed to reduce the health risk associated with excess accumulation of body fat, as measured by change in BMI, may be prone to misinterpretation.
Let’s illustrate this point by example. The body mass for a 1.8m tall adult man of ‘Normal’ BMI could range from 60kg for a BMI of 18.5 to 81kg for a BMI of 25, a difference in mass of 21kg! This suggests the abilty of BMI to predict ‘normal’ body mass is quite limited. Equally, BMI cannot predict how much of the body mass is fat nor location of fat around the body, the two primary links to health risk. In the worst case scenario for this subject starting at a body mass of 60kg, he could accumulate 21kg of excess fat mass over time but, assessed by BMI still be considered ‘normal’ and thereby of low health risk. Extension of this example to a BMI equivalent to overweight and obese is equally startling.
A large proportion of the research expertise within the PESS department engage in investigation of factors relating to the two principal components affecting body fat, i.e. energy intake and energy expenditure. Common to all is the accurate determination of human body composition, i.e. fat, lean, bone and water mass. In professional practise, estimates of body composition (principally fat and non-fat mass) are derived from algorithms generated by the measurement of skinfold thickness at representative sites (compartments) of the human body. The validation of the algorithms and population specify range of ‘norms’ within Europe is based upon data collected from a British population of only 481 subjects aged 16-72y in 1974. Astonishingly, these algorithms, clearly not representative of the population of Ireland today, have not been revised.
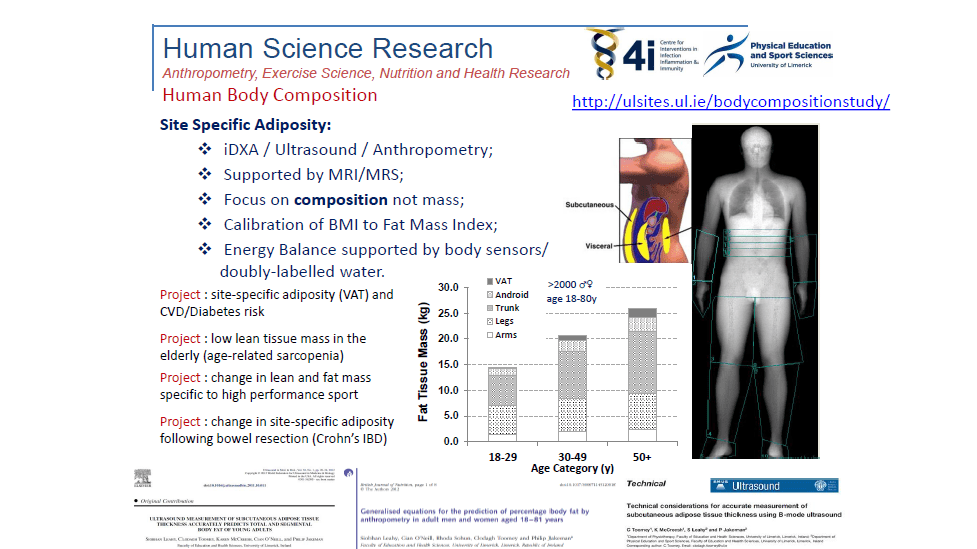
Using the latest technologies to measure accurately whole body and regional distribution of fat and lean tissue mass and the University and local community as representative of the Irish population we have conducted a survey of body composition and presented these findings stratified by age and sex. These data underpin future intervention studies designed to reduce obesity and other health risks related to aberrant body composition in the Irish population. We have also applied the same technology to assist in the development of optimal body composition, fat and lean mass, for a wide range of high performance athletes, Senior County GAA and Irish and Munster Rugby players. Recognising the paradoxical rise in the incidence of poor bone health of female athletes researchers are also exploring why this occurs and what can be done to prevent it.
You can find out more about this work and how you might contribute at http://ulsites.ul.ie/bodycompositionstudy/
Phil Jakeman is a Professor of Sport and Exercise Sciences here in the PESS Department at the University of Limerick. View Phil’s profile Here!
Phil’s Email: phil.jakeman@ul.ie
Discover more from PESS News & Information
Subscribe to get the latest posts sent to your email.
