
This blog post gives a brief overview of the infamous sampling technique in sport science and exercise physiology circles known as the muscle biopsy. Many (under)graduate students will have “earned their stripes” by taking part in nutrient and exercise interventions using biopsies. So, why do we do it? This post will give an overview of the history of the biopsy, the development of the technique, as well as some commentary on the sampling methodologies and some considerations for exercise physiology research. For this post, I have leaned heavily on Bjorn Ekblom’s (Astrand Laboratory, Swedish School of Sport and Health Sciences) review article which you should check out here* https://onlinelibrary.wiley.com/doi/full/10.1111/sms.12808 and a recent publication form our group led by Dr Robert Davies (PESS) which you can read in full here* https://onlinelibrary.wiley.com/doi/abs/10.1111/sms.13295
Brief History and Technique Development
The modern technique suitable for human sampling was originally described in a paper by Bergstrom in 1962, however, it seems muscle biopsies were already being used by other labs at this point with biopsies mentioned in papers by Harrison (1952) and Reiffel and Stone (1957). Bergstrom is credited with the development of the technique as he described the method, the use of the needle and some potential clinical applications of the muscle biopsy. The needle he describes is referred to as the “Bergstrom needle” (Figure 1). Others favoured the use of the Weil-Blakesley conchotome (Figure 2) while more recently, many researchers have moved toward a minimally invasive microbiopsy procedure first described by Hayot and colleagues in 2005 (here http://erj.ersjournals.com/content/25/3/431.long).
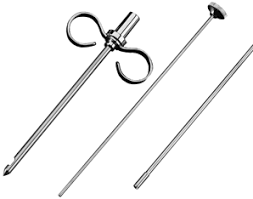
Figure 1. Bergstrom needle (outer cylinder, inner cylinder, rod)

Figure 2. Weil-Blakesley conchotome

Figure 3. Microbiopsy needle
Comparison of methodologies
The Bergström needle consists of two cylinders. The outer cylinder is 3-5 mm in diameter with a window near the tip (Figure 1) where muscle tissue bulges into the window. By pushing down the smaller inner needle through the outer one, the sharp inner needle cuts the tissue that bulges in through the window like a guillotine. Up to 80 mg of muscle tissue can easily be extracted but sometimes suction is added to increase the tissue which bulges into the window, and thus increases the tissue yield. The Weil-Blakesley conchotome consists of an alligator forceps that opens with a scissor grip. Typically 80 mg of muscle tissue is extracted with larger conchotomes. Ekblom suggests that the small conchotome causes less discomfort during the procedure and less pain the day after a muscle biopsy while enough muscle tissue can still be extracted. The microbiopsy procedure which has recently become more prominent, is less invasive, as in contrast to the other two procedures no incision is required. A 14-18 guage needle (Figure 3) can be used, similar in principle to the Bergstrom, but using a spring-loaded trigger mechanism, these needles can obtain up to 55 mg of tissue which is sufficient to carry out most analyses. Most models tend to be disposable, which is considered an advantage, as both the Bergstrom and Weil-Blakesley conchotome require sterilisation by autoclave before re-use. A combination of these factors has led to the adoption of this technique in more and more labs recently.
Value of the muscle biopsy
The development of the muscle biopsy technique significantly advanced research in the area of exercise and nutrition physiology. Bergström and Hultman were the first to publish more detailed data regarding muscle metabolism using the needle biopsy technique. They showed in a series of excellent experiments how muscle glycogen concentration changed with exercise and how the glycogen concentration could be rebuilt by nutritional interventions. Legends of the field such as Dave Costill, Bengt Saltin, John Holloszy described the effects of distance running on glycogen concentrations in different fibre types, enzymatic content of trained and untrained muscles and mitochondrial biogenesis in response to training. Without the biopsy technique, we would be unable to define the “omics” of muscle and the mechanisms through which muscle adapts to both exercise and nutrition.
Considerations
A major consideration in muscle biopsy studies is the location of the muscle being sampled, as this has implications for fibre types as well as the use of that muscle during exercise. Proximal to distal effects are prevalent as well as the depth of the muscle tissue sampled. A further unwanted effect of muscle biopsies is that the penetration into the muscle can cause a sterile inflammatroy reaction in the region. Therefore, it is recommended that when several biopsies are taken in an experiment, there should be a 2-cm proximal gap between biopsies to avoid the inflammatory influence of a previous biopsy.
Recently, we studied the effects of a previous muscle microbiopsy on static and dynamic muscle function. This study, led by Dr Robert Davies at the PESS department demonstrated that a previous muscle biopsy causes a reduction in peak force and rate of force development during an isometric squat with a shift in force from the biopsied to the non-biopsied limb (Figure 4). A reduction in ground reaction force during and in landing from a countermovement jump was also evident (Figure 5). At the time of publication this paper created some mild debate on social media, with other researchers (Prof Stu Phillips, Dr Leigh Breen) suggesting the skill of the clinician who extracted the biopsies could have an influence. We use medical doctors to undertake these experiments and both have experience of >200 biopsies between them. Interestingly, Stu and Leigh come from labs with experience of taking in excess of 15,000 biopsies, which is quite an achievement! Participants did report mild pain and discomfort post biopsy, but there was no correlation between the level of pain and reduction in force observed. There were also no complications with these biopsies, so we do not believe the experience of our clinicians was a factor here. However, we believe this is an important consideration for the design of future studies which intend to measure force post-biopsy, as a reduction may be evident as a result of the sampling technique.

Figure 4. Isometric Squat force‐time trace. Pre‐biopsy (gray line) and post‐biopsy (black line) isometric squat (ISQ) bilateral force‐time trace from a typical subject. Corresponding dashed lines signify the change (Δ) pre‐ (gray) to post‐biopsy (black) for peak isometric force (PIF) and the rate of force development (0‐150 ms; rate of force development)

Figure 5. Countermovement Jump force‐time trace. Prebiopsy (gray line) and post‐biopsy (black line) countermovement jump (CMJ) bilateral force‐time trace from a typical subject. Corresponding dashed lines signify the change pre‐ (gray) to postbiopsy (black) for CMJ variables (ground reaction force (A), peak force (B), average force (C), flight time (D))
*If you cannot access these articles, please get in touch with brian.carson@ul.ie
Dr Brian Carson is a Lecturer in Exercise Physiology and course director for the BSC Sport and Exercise Sciences programme in the Department of Physical Education & Sport Sciences at the University of Limerick. Brian’s current research interests are investigating the association between physical activity behaviours and metabolic health with a specific focus on metabolic flexibility and how physical activity interventions can monitor these outcomes. Contact Brian via email at Brian.Carson@ul.ie or view his research profile on Researchgate. 
Discover more from PESS News & Information
Subscribe to get the latest posts sent to your email.
